The rotator cuff covers the anterior, posterior, and upper surfaces of the humeral-scapular joint. The rotator cuff (hood)is a group of muscles that surround, like the hood, the head of the humerus. We distinguish 4 muscles that make up the rotator cuff: the subscapular, supraspinous, and infraspinous muscles and one smaller, which is much less damaged: the tendon of the minor muscle.
In this article, Niketrainers.com.co will tell you:
Function of Rotator cuff
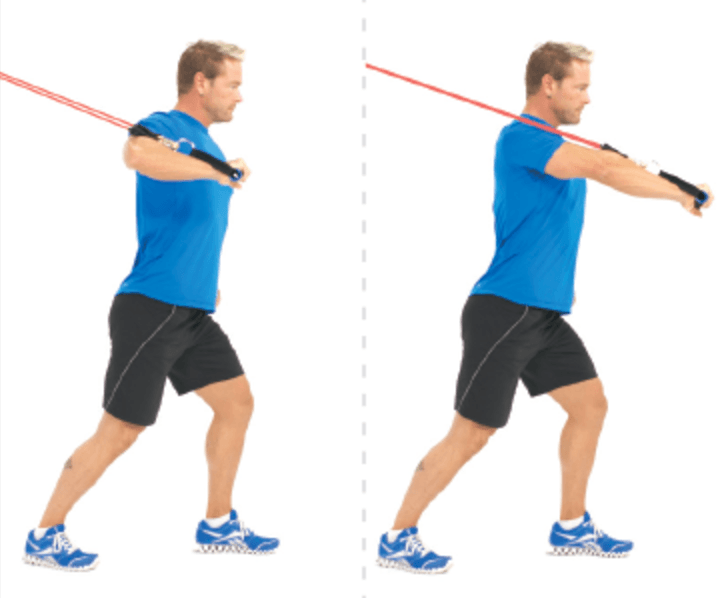
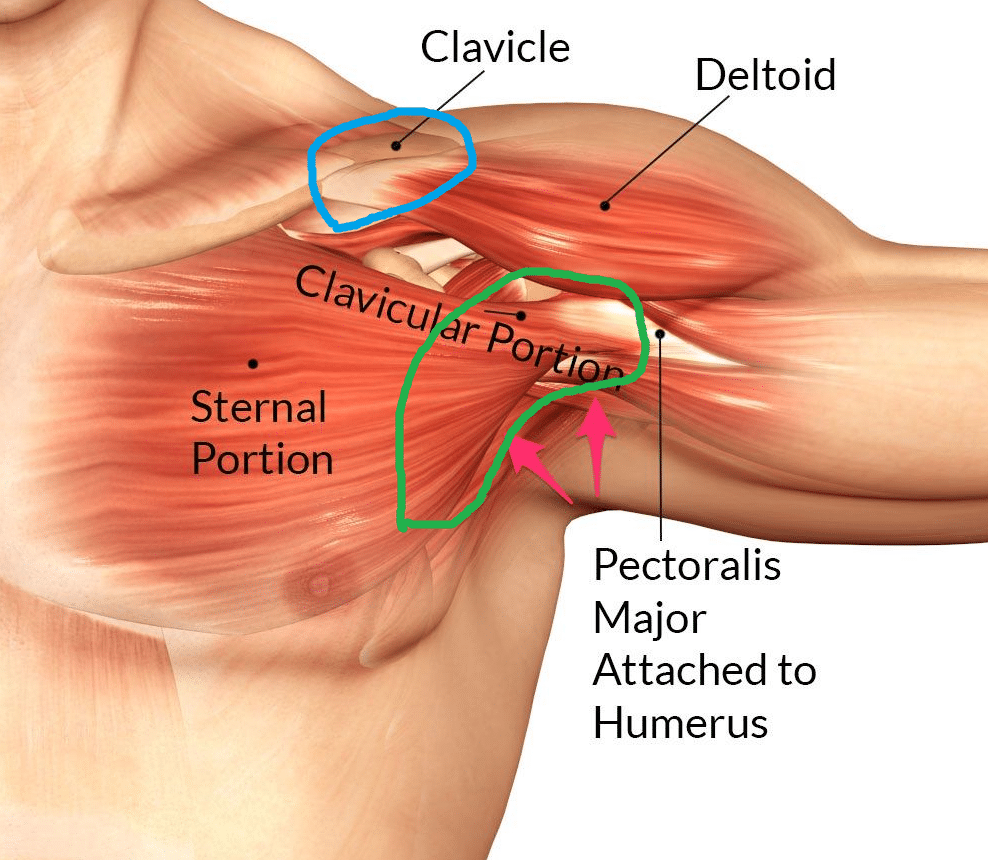
The main function of the rotator cuff is to stabilize the head of the humerus in the acetabulum and initiate movement in the humerus (abduction and flexion movements). He is the strongest initiator of the movement. It is responsible for the first 20-30% of the Abduction movement (down to about 20 degrees), then the deltoid muscle is taken over by the upward movement of the arm. Thus, for hand movement in the shoulder joint to be possible, the rotator cuff must interact with the deltoid muscle. In addition, the rotator cuff is responsible for rotational movements in the shoulder joint (hence its name). These are the movements of external and internal rotation.
The causes of the Rotator cuff Tear
- degenerative (overload)
The dysfunction of the rotator cuff tendon and the supraspinatus tendon leads to a muscle imbalance causing the humeral head to sublux upwards. Then, there is a narrowing of the sub-brachial space, filled with the bursa, and thus the symptoms of subacromial conflict, i.e. the collision of the rotator cuff attachment with the appendix. The sub-chin conflict contributes to damage to the degenerative (overload) rotator cuff. As a result of chronic microtrauma, changes in the tendon occur, leading to its rupture.

The sub-brachial bursal conflict is usually accompanied by inflammation of the sub-brachial bursa. Often, the damage to the cone itself is associated with inflammation. Sometimes, especially in young people, with taper dysfunction, bursitis occurs in the absence of mechanical damage to the rotator cuff. In this situation, exercises to strengthen the rotator cuff help stabilize the head of the humerus in the acetabulum and heal the patient. Untreated, long-lasting sub-shoulder conflict against the background of a torn rotator cuff leads to degenerative changes (arthrosis) in the shoulder joint. Shoulder arthrosis is painful and difficult to treat, it can cause complete dysfunction of the shoulder joint, requiring replacement of the joint with an endoprosthesis.
Muscle imbalance in the rotator cuff that can lead to a subacromial conflict often occurs in people over the age of 50 and for no specific cause. Due to age, there are atrophic changes in the tendons of the rotator cuff. Also in young people, especially those exercising incorrectly in the gym, there may be a muscle imbalance. These people often over-exercise the deltoid muscle and neglect the exercise of the rotator cuff muscle.
An interesting paradox is the fact that a large proportion of people aged 50-60, despite the lack of symptoms, have a damaged or torn rotator cuff. It is the result of degenerative changes in the tendon that progress with age. An asymptomatic rotator cuff injury is not eligible for surgery. In comparison, in the case of people who have injured the rotator cuff as a result of an injury, the degree of taper damage may be less than in the elderly, who do not have symptoms, but people after an injury may have very severe and bothersome symptoms. Such cases qualify for surgery.
The group most exposed to degenerative damage to the rotator cuff are people who perform repetitive overhead activities (interior painters, baseball players, basketball players, volleyball players). People who train intensively in the gym, especially those working on strengthening the deltoid muscle, rather than strengthening the rotator cuff, lead to muscle imbalance, which can also damage the rotator cuff.
- injury
Injury of the rotator cuff occurs in younger people, under 60 years of age, as a result of a sudden jerk of the arm in a rotating motion. Other movements that cause this injury include: sudden grasping, twisting the arm, hanging on the hands, etc. Often, traumatic damage to the rotator cuff occurs when a car driver tries to reach for a heavy bag that lies behind the seat. Unable to lift it easily, she tugs at it, and often the attachment of one or more tendons of the rotator cuff is ruptured.
Symptoms Rotator cuff – How do I know if I have rotator cuff injury?
With degenerative damage to the rotator cuff, the disease is cyclical, i.e. exacerbations periodically occur, during which patients experience:
- pain located in 1/3 of the proximal arm. Pain occurs after overload, periodically there may be night pains. Sometimes there are diffuse pains caused by inflammation of the subacral bursitis.
- muscle weakness (weaker arm, feeling that you don’t have the strength to raise your arm)
- symptom of a painful arch (a symptom characteristic of a subacromial conflict), i.e. pain that occurs in the middle phase of the shoulder abduction (from 30 to about 120 degrees) and disappears at the end of the movement.
In massive injuries of the rotator cuff, pseudoparalysis may occur. The patient is unable to make any hand movements.
In the event of an injury, patients experience a sharp pain throughout the shoulder. After the first acute symptoms of trauma have been extinguished, the pain changes its specificity and is similar to the pain occurring in degenerative damage to the cone, i.e. it is located in 1/3 of the proximal humerus. This pain is also accompanied by other symptoms characteristic of degenerative damage to the rotator cuff.
Diagnostics Rotator cuff Tear
- clinical examination by an orthopedist
- medical interview
- imaging tests:
⇒ magnetic resonance imaging with or without contrast
The best diagnostic results are obtained with contrast magnetic resonance imaging (arthrography). It is a very thorough examination, which gives a high probability of correct diagnosis of rotator cuff damage
⇒ x-ray
Unfortunately, the X-ray result does not always clearly indicate damage to the rotator cuff, which is why the MRI test is definitely more recommended.
An ultrasound can also be performed, but for it to be of diagnostic value, it must be performed by an experienced ultrasound specialist who will be able to arrange the hand in such a way as to be able to see the rotator cuff. The difficulty in assessing the rotator cuff in ultrasound is due to the fact that the cone is covered with a bone part (the shoulder process).
Qualification for surgery should take place after performing all three diagnostic elements (physical examination, medical history and imaging tests). A common mistake is to qualify patients for surgery only on the basis of one of the diagnostic elements, e.g. only on the basis of the results of magnetic resonance or X-ray.
The decision on the type of treatment depends on the degree of damage to the rotator cuff, the frequency of symptoms and their severity.
Conservative treatment of Rotator cuff Tear
The type of conservative treatment depends on the severity of the pain. In people with very severe pain, caused very often by the accompanying bursal bursitis, in the first phase of treatment, the inflammation of the subacromial bursa should be extinguished and the pain should be reduced.
The following are used: immobilization in a sling, oral analgesics and non-steroidal anti-inflammatory drugs, anti-inflammatory and anti-swelling ointments, cooling, physical therapy (cryotherapy and anti-inflammatory iontophoresis, electrostimulation of the rotator cuff muscles). If the pain persists despite the use of oral painkillers, steroid injections (blockade) can be used. However, you should avoid administering steroid injections more than 2 times, as steroids administered to the subacial cavity in excess may damage the rotator cuff. In the second phase, exercises are recommended to strengthen the rotator cuff and restore movement (kinesiotherapy).
By using appropriately selected exercises, the head of the humerus in the acetabulum is stabilized (it pulls the head to the correct position, i.e. down), thus restoring the muscle balance.
Conservative treatment is used in people:
- with minor pain
- with degenerative damage to the rotator cuff
- in the elderly (women over 55 and men over 65) who suffer an injury, conservative treatment is also tried at the beginning. Only after the failure of conservative treatment, surgery is proposed.
Surgery Rotator cuff Tear
Indications for surgery depend on the degree of damage, age, severity of symptoms and previous treatment. However, it is assumed that surgical treatment should be applied:
- in patients with pseudoparalysis. In these patients, conservative treatment in the form of exercise does not make sense as they are unable to move their arms and are unable to perform any exercises.
- in women up to 55 years of age and men up to 65 years of age with traumatic damage to the rotator cuff. In women and men above this age limit, the decision to operate depends not on the record age, but on biological age. The determinants of biological age are: physical fitness, the form in which the patient is and the level of life activity. The better shape, more fit and active a person is, the lower their biological age is, and the more justified is the qualification for surgical treatment.
- in patients with degenerative damage to the rotator cuff, in whom, despite physical therapy lasting 2-3 months to six months, no improvement was achieved.
When deciding whether to use surgical treatment, the degree of damage to the rotator cuff is also an exponent. The damage may be:
- total
Then, the attachment of one of the muscles forming the rotator cuff (usually the supraspinatus tendon) is completely broken. The muscle detached from the attachment site contracts and “escapes”.
If the decision to treat is delayed for too long, this muscle will also atrophy (unused muscle atrophies). There are three degrees of muscle wasting atrophy:
I – partial atrophy of about 1/3 of the belly of the muscle
II – atrophy from 1/3 to 2/3 of the belly of the muscle
III – atrophy of more than 2/3 of the belly of the muscle

In the third stage, attempts are made to reconstruct the tendon. However, there is a risk of failure due to the fact that the tendon may become so contracted and so atrophied that it cannot be pulled to the attachment point. In addition, the belly of the muscle may be contracted to such an extent that, despite the tendon being sewn to the attachment site, the belly will not perform its function.
Therefore, it is extremely important not to delay the decision on surgery until the last minute.
- partial
The continuity of the tendon is maintained, but delamination, i.e. partial damage, occurs. The rotator cuff tendon is thick, looking like it is composed of two layers on top of each other. Delamination is the tearing / delamination of some layers of the tendon.
In patients who have experienced delamination, despite the undertaken rehabilitation attempts, it is most often impossible to regain the efficiency of the rotator cuff and stabilize the humeral head. Therefore, the best solution in the case of delamination is surgery.
There are two types of partial damage:
- Damage from the side of the sub-shoulder bursa (sub-shoulder space)
- Secondary damage
- Intratiginous lesions

Surgical treatment is divided into three groups:
- reconstruction of the tendons of the rotator cuff
- latissimus dorsi muscle transplant
- shoulder prosthesis
Rotator cuff tendon reconstruction
The surgery for the reconstruction of the rotator cuff tendons (sewing them back in place of the attachment) can be performed using the arthroscopic method and open-ended. Open procedures are rarely performed at the moment, despite the fact that, if properly performed, they have results comparable to arthroscopic surgery. The advantage of the arthroscopic technique is that during arthroscopy it is possible to identify and repair concomitant pathologies (most often these are biceps pathologies and sub-chin conflict). In addition, operations performed using the arthroscopic technique are less burdensome for the patient.
The arthroscopic surgery starts with making a few small incisions around the shoulder joint. A camera is inserted through one of these incisions, the others are used for inserting tools during operating procedures. Both in the open method and in the procedures performed with the arthroscopic method, the surgeon refreshes the attachments. Refreshing is by causing bleeding (“cuts”) to the bones and tendons. Blood initiates repair processes, bleeding tissue has a better healing potential (each healing process begins with bleeding). Then the orthopedic surgeon, using special anchors (screws) with threads, sews the tendon into the spongy part of the bone (this part of the bone has great regenerative capacity).
Latin dorsal muscle transplant
The operation consists in collecting the peripheral tendon attachment. Then the attachment is moved to the place of the rotator cuff attachment (to the head of the humerus). Its purpose is to replace the function of the rotator cuff.

Shoulder prosthesis
Shoulder replacement surgery is used when there is a massive degenerative lesion or when it is suspected that the transplant of the latissimus dorsi muscle will be unsuccessful.
The latissimus dorsi muscle transplant and shoulder prosthesis implantation are used in the case of very large damage to the rotator cuff, when it is not possible to sew the taper tendons in place of the attachment, or when the reconstruction of the rotator cuff tendons was ineffective. These operations are rarely performed.
Approximate time of the procedure:approx. 1.5-3 hours
Type of anesthesia:general endotracheal
Hospital stay: The patient comes to the hospital on the day of surgery. All examinations and an anaesthesiological consultation are performed earlier. The day after the operation, if there are no complications, the drain is removed, the patient receives rehabilitation instruction and is discharged home.